Patellar Tacking Disorder
- Asiyah Patel
- 14 hours ago
- 6 min read


Patellar tracking disorder, also known as patellar maltracking, refers to abnormal movement of the patella (the kneecap). Normally the patella glides smoothly in a groove at the end of your thigh bone (trochlear groove) when you bend or straighten the knee. When this movement is not smooth or unbalanced, a spectrum of disorders, from malalignment to recurrent patella instability and dislocation can occur. It most commonly affects young individuals, particularly women, and is frequently associated with anterior knee pain. If left undiagnosed, chronic maltracking can progress to patellofemoral cartilage damage and early osteoarthritis.
Anatomy of the Patellofemoral Joint
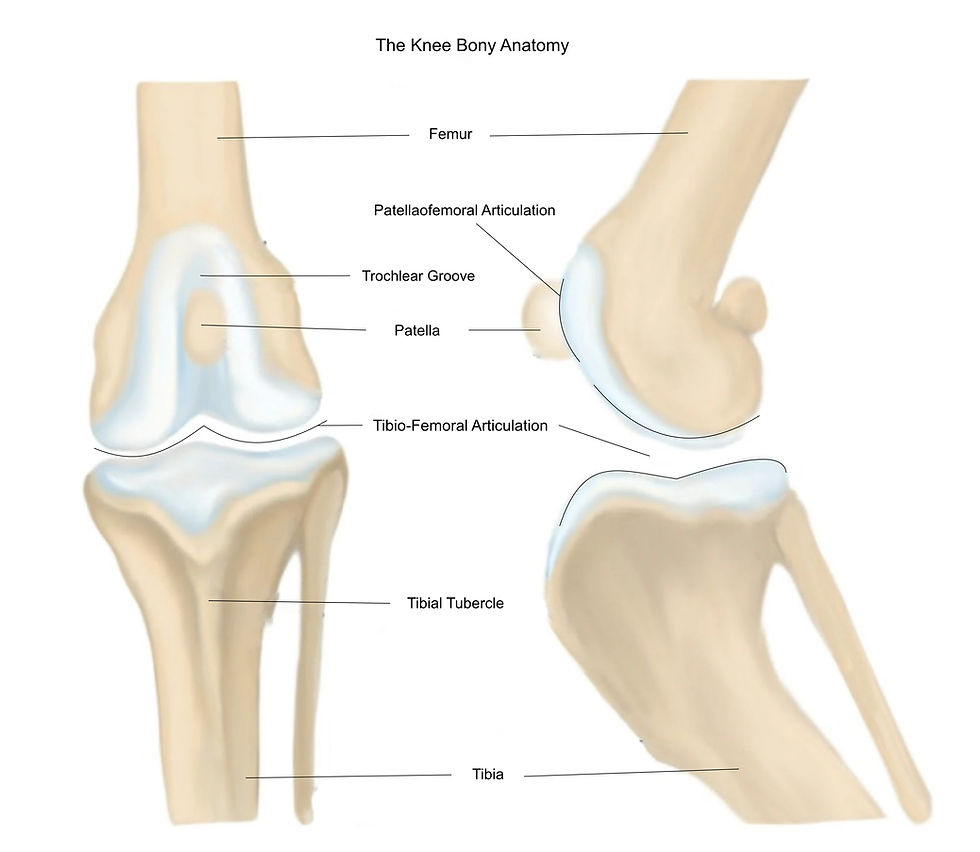
The knee joint is made of 3 bones, the femur, the tibia and the patella. These bones interact with each other, making a tibio-femoral articulation, and a patellaofemoral articulation.
The patella is shaped like an inverted triangle and lies within the quadriceps tendon, which connects the quadriceps muscles of the thigh to the lower leg. This tendon continues below the patella as the patellar tendon, which attaches to the tibial tubercle on the tibia. This arrangement allows forces by the quadriceps muscles to be transmitted across the knee joint to extend the leg called the extensor mechanism.

The back (posterior) surface of the patella, which articulates with the femur, is divided into two main articular regions: a medial facet and a lateral facet, separated by a vertical ridge.
The patella articulates with the trochlear groove. This groove forms a channel that guides the patella during knee movement. This groove contains corresponding medial and lateral articular surfaces that match the patellar facets. Typically, the lateral trochlear surface is more prominent than the medial side, which helps prevent the patella from moving too far toward the outside of the knee, known as patellar displacement. When the knee bends (flexion) or straightens (extension), the patella moves up and down within this groove. The depth and shape of the trochlear groove help keep the patella centred and prevent it from moving excessively to either side.
How the Patella moves through knee movement
As the knee moves from extension to flexion, the area of contact between the patella and the femur changes. In full extension, the patella has little or no contact with the trochlear groove, which makes it more vulnerable to instability. When the knee flexes to approximately 10–20°, the patella begins to engage within the trochlear groove. As flexion increases, contact area is more proximal on the patella. When the knee flexes beyond 90°, the lateral facet contacts the femur, contributing to load distribution. Additionally, the quadriceps tendon also comes into contact with the trochlear groove, further distributing forces.
The patella moves in four planes of direction:
· Flexion and extension
· Medial and lateral rotation
· Medial and lateral tilt
· Medial and lateral translation (shift)
Patellar stability depends on both the bony anatomy of the joint and the surrounding longitudinal and transverse soft-tissue stabilising structures.

The transverse stabilisers include the medial and lateral retinacula, the vastus medialis and vastus lateralis muscles, the iliotibial band, and the medial patellofemoral ligament (MPFL). These structures help control side-to-side motion and tilt of the patella. The longitudinal stabilisers, the quadriceps tendon and the patellar tendon which make the extensor mechanism, also stabilise the patella. The alignment between the force generated by the quadriceps muscles and the direction of pull of the patellar tendon is described by the Q angle, which normally measures 10–15° of valgus. This angle produces a slight upwards and sideways pull on the patella by the quadriceps. As a result, during the early phase of knee flexion, the patella must move slightly medially in order to properly engage the trochlear groove.
What Causes Patella Maltracking
Several structural and biomechanical abnormalities contribute to abnormal patellar motion.
Trochlear dysplasia
Abnormal flattening of the trochlear groove reduces the bony constraint that normally guides the patella.
Patella alta
Here the patella sits higher than normal. Engagement with the trochlear groove occurs later in knee flexion, increasing the risk of instability.
Increased tibial tubercle–trochlear groove (TT–TG) distance
When the tibial tubercle sits more laterally, the line of pull of the patellar tendon also becomes more lateral, producing a lateral force on the patella.
Soft-tissue imbalance
Injury or laxity of the MPFL and medial retinaculum decreases resistance to lateral displacement. Conversely, tightness of the lateral retinaculum increases lateral tilt, also increasing chance of displacement.
Muscular dysfunction
Weakness or delayed activation of the vastus medialis obliquus (the quadriceps muscle on the inner thigh) relative to the vastus lateralis (the quadriceps muscle on the outer thigh) may further contribute to lateral patellar tracking.
Clinical Presentation

Patients with patellar maltracking commonly present with:
Anterior knee pain
Sensations of instability or giving way
Mechanical symptoms such as clicking or popping
Pain during activities including squatting, stair climbing, or prolonged sitting
Recurrent lateral patellar dislocations.
Diagnosis relies on a combination of clinical assessment and MRI imaging.
Nonoperative management
Initial treatment commonly focuses on conservative management. Physiotherapy focused on quadriceps strengthening, particularly the vastus medialis, hip and core stabilisation exercises. This allows the appropriate structures surrounding the joint to contribute to the stabilisation of the patella and minimises abnormal movement.
Some exercises include:
· Straight Leg Raises
· Terminal Knee Extensions
· Wall Sqauts
· Clamshells
· Side-lying Leg Raises
Surgical management
Surgical treatment is considered in cases of recurrent instability, persistent symptoms, or significant structural abnormalities.
Procedures are selected based on the underlying anatomical pathology:
Medial patellofemoral ligament reconstruction
Reconstruction of the MPFL restores the primary soft-tissue restraint to lateral patellar displacement.
Tibial tubercle osteotomy
Medialisation of the tibial tubercle can correct abnormal alignment or patella alta by altering the direction of the patellar tendon force.
Trochleoplasty
In severe trochlear dysplasia, reshaping of the trochlear groove may be performed to improve patellar containment.
Conclusion
Patellar maltracking is a complex disorder involving abnormalities in the bony anatomy and the soft-tissues within and surrounding the patellofemoral joint. Key anatomical contributors include trochlear dysplasia, patella alta, increased TT–TG distance and muscular dysfunction. People who suffer from Patella maltracking often experience knee pain and instability requiring accurate diagnosis and management to mitigate pain. Management ranges from conservative rehabilitation strategies that aims to increase muscular strength to stabilise the patella, to targeted surgical correction for the underlying anatomical abnormalities.
References:
Amis, A. A., Firer, P., Mountney, J., Senavongse, W., & Thomas, N. P. (2003). Anatomy and biomechanics of the medial patellofemoral ligament. Knee, 10(3), 215–220. https://doi.org/10.1016/S0968-0160(03)00006-1
Buckens, C. F. M., & Saris, D. B. F. (2010). Reconstruction of the medial patellofemoral ligament for treatment of patellofemoral instability: A systematic review. The American Journal of Sports Medicine, 38(1), 181–188. https://doi.org/10.1177/0363546509353132
Fithian, D. C., Paxton, E. W., Stone, M. L., Silva, P., Davis, D. K., Elias, D. A., & White, L. M. (2004). Epidemiology and natural history of acute patellar dislocation. The American Journal of Sports Medicine, 32(5), 1114–1121. https://doi.org/10.1177/0363546503260788
Freepik. (n.d.). Young sport woman suffered from knee pain injury while running city [Image]. https://www.freepik.com/free-photo/young-sport-woman-suffered-from-knee-pain-injury-while-running-city_30236420.htm#fromView=search&page=1&position=0&uuid=f327bf0a-963a-4ac5-b1c0-a07152fa412e&query=knee+pain">Image.
Freepik. (n.d.). leg with knee pain [Image]. https://www.freepik.com/free-photo/leg-with-knee-pain_922812.htm#fromView=search&page=1&position=30&uuid=25199dd2-43d6-46f4-906e-75fa348548e3&query=kneecap+pain.
Horton, M. G., & Hall, T. L. (1989). Quadriceps femoris muscle angle: Normal values and relationships with gender and selected skeletal measures. Physical Therapy, 69(11), 897–901. https://doi.org/10.1093/ptj/69.11.897
Jibri, Z., Jamieson, P., Rakhra, K. S., Sampaio, M. L., & Dervin, G. (2019). Patellar maltracking: An update on the diagnosis and treatment strategies. Insights into Imaging, 10(1), 65. https://doi.org/10.1186/s13244-019-0755-1
Lewallen, L., McIntosh, A., & Dahm, D. (2015). First-time patellofemoral dislocation: Risk factors for recurrent instability. The Journal of Knee Surgery, 28(4), 303–309. https://doi.org/10.1055/s-0034-1398373
Nakagawa, S., Kadoya, Y., Kobayashi, A., Tatsumi, I., Nishida, N., & Yamano, Y. (2003). Kinematics of the patella in deep flexion: Analysis with magnetic resonance imaging. The Journal of Bone and Joint Surgery, 85(7), 1238–1242. https://doi.org/10.2106/00004623-200307000-00009
Tecklenburg, K., Dejour, D., Hoser, C., & Fink, C. (2006). Bony and cartilaginous anatomy of the patellofemoral joint. Knee Surgery, Sports Traumatology, Arthroscopy, 14(3), 235–240. https://doi.org/10.1007/s00167-005-0683-0
Wechter, J., Macalena, J., & Arendt, E. A. (1994). Lateral patella dislocations: History, physical exam, and imaging. In R. V. West & A. C. Colvin (Eds.), The patellofemoral joint in the athlete (pp. 15–29). Springer.
Zhang, G. Y., Zheng, L., Ding, H. Y., Li, E. M., Sun, B. S., & Shi, H. (2015). Evaluation of medial patellofemoral ligament tears after acute lateral patellar dislocation: Comparison of high-frequency ultrasound and MR. European Radiology, 25(1), 274–281. https://doi.org/10.1007/s00330-014-3407-3
Assessed and Endorsed by the MedReport Medical Review Board