Endometriosis and Infertility: More than just "really bad period cramps"
- Samantha Sutherland

- Mar 24
- 4 min read

Introduction
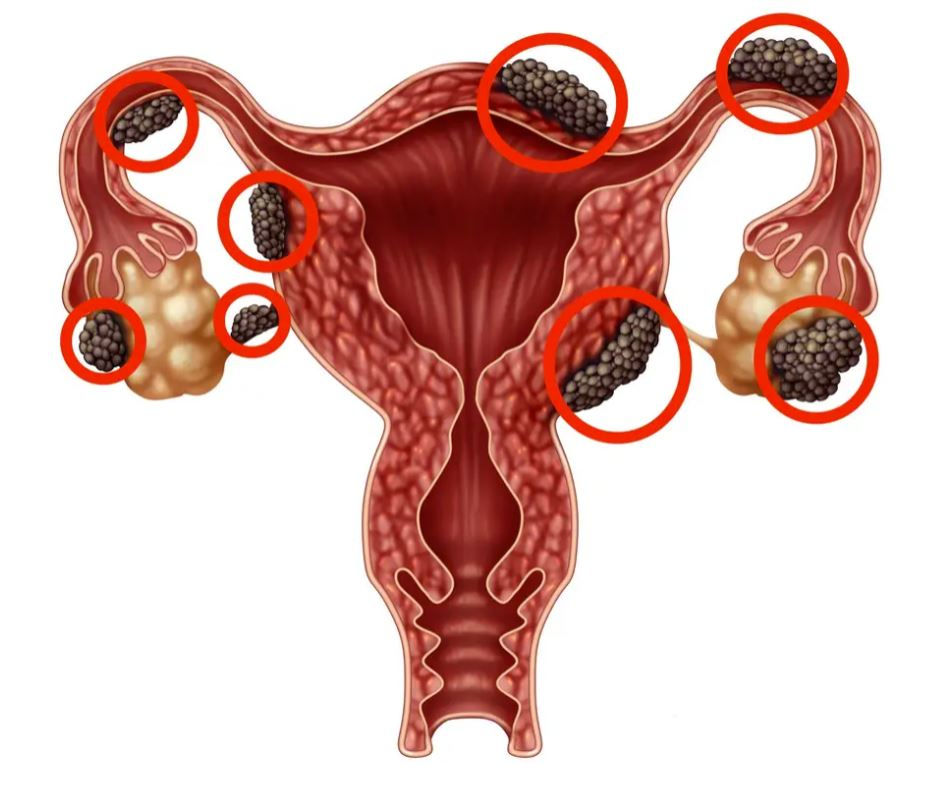
Endometriosis occurs when cells like those of the endometrial lining implant and grow outside the uterus, most commonly on the ovaries, fallopian tubes, and peritoneal surfaces. These ectopic implants respond to hormonal cycles, leading to inflammation and scar tissue formation. Since the disease depends on estrogen and involves inflammation, it’s most often diagnosed in women aged 25–35.
Although endometriosis is diagnosed in 10-15% of women, with 30-50% of diagnosed individuals experiencing infertility and a significant impact on quality of life; diagnosis is challenging because symptoms mimic other disorders. A definitive diagnosis typically requires laparoscopy, a surgical procedure that directly visualizes pelvic organs. Non-invasive imaging (e.g., ultrasound, MRI) helps suggest the diagnosis but may miss subtle cases.
Causes and Pathogenesis
While the exact cause of endometriosis remains unknown, multiple theories explain its development:
Retrograde Menstruation
Sampson’s theory proposes that menstrual blood containing viable endometrial cells flows backward through the fallopian tubes into the pelvic cavity, where the cells implant and proliferate. Retrograde menstruation occurs in most women, but in those with endometriosis, immune and cellular abnormalities may permit ectopic implantation.
Coelomic Metaplasia
According to this theory, the cells lining the pelvic cavity can transform into endometrial-like cells under certain stimuli, explaining endometriosis in locations far from the uterus.
Immune and Inflammatory Dysfunction
Women with endometriosis often have altered immune responses that fail to clear misplaced endometrial cells. Elevated inflammatory cytokines in the peritoneal fluid can foster lesion growth and pelvic inflammation.
Stem Cells and Genetics
Emerging evidence suggests that bone-marrow derived stem cells might differentiate into endometrial tissue at ectopic sites. Genetic and epigenetic factors also contribute to disease susceptibility.

Symptoms
The clinical presentation of endometriosis is diverse, ranging from asymptomatic to debilitating. Common symptoms include:
Dysmenorrhea (painful periods)
Chronic pelvic pain
Dyspareunia (painful intercourse)
Heavy menstrual bleeding
Bladder or bowel symptoms related to lesion location
Some women experience no pain yet struggle with infertility.
Endometriosis and Infertility
Epidemiology of Infertility in Endometriosis
Infertility is more common in women with endometriosis than in women without it, and endometriosis is found in up to half of women undergoing evaluation for infertility.
Endometriosis impacts fertility through multiple mechanisms:
Pelvic Adhesions and Anatomical Distortion
Inflammation and scarring can distort pelvic anatomy, obstruct fallopian tubes, and impair the normal movement of eggs and sperm. This mechanical disruption can prevent fertilization.
Endometriomas
These ovarian cysts (sometimes called “chocolate cysts”) produce local inflammation and oxidative stress, which can damage ovarian follicles, reduce ovarian reserve, and impair ovulation.
Inflammatory and Hormonal Environment
Peritoneal and follicular fluid in women with endometriosis often contains inflammatory cytokines and oxidative molecules that can damage gametes (oocytes and sperm) and early embryos.
Impaired Endometrial Receptivity
The normal uterine lining must be receptive during a narrow “implantation window” for pregnancy to occur. In endometriosis, molecular alterations (e.g., aberrant progesterone signalling and gene expression such as HOXA10) can reduce receptivity and prevent implantation.
Pain-related Sexual Dysfunction
Pain during intercourse can reduce intercourse frequency, indirectly contributing to sub-fertility.

Treatment of Endometriosis
Pain Management and Symptom Control
- Medical therapy (e.g., hormonal contraceptives, progestins, GnRH analogs) often reduces pain and suppresses lesion activity but does not improve fertility and may delay attempts to conceive.
Surgery
- For selected patients, especially those with minimal to mild disease—laparoscopic removal of implants can improve natural pregnancy rates by restoring anatomy and reducing inflammation.
Assisted Reproductive Technologies (ART)
- In vitro fertilization (IVF) is the most effective fertility-enhancing option for women with endometriosis, particularly in moderate to severe cases or when other infertility factors coexist. IVF bypasses many mechanical and physiological barriers.
Fertility Preservation
- Since endometriosis and its treatments can threaten ovarian reserve, fertility preservation (oocyte or embryo cryopreservation) may be considered for some patients, especially if delaying pregnancy is anticipated.
Conclusion
Endometriosis is a complex condition that can affect fertility in many ways, even in individuals with mild or no symptoms. Inflammation, hormonal changes, and structural damage within the pelvis can interfere with ovulation, fertilization, and implantation. Since the condition varies widely from person to person, treatment should be individualized and guided by both symptom severity and fertility goals. While hormonal therapies help manage pain, surgical treatment and assisted reproductive technologies are often more effective options for those trying to conceive. Continued research is needed to improve diagnosis and fertility outcomes for people living with endometriosis.
References
Bonavina, G., & Taylor, H. S. (2022). Endometriosis-associated infertility: From pathophysiology to tailored treatment. Frontiers in Endocrinology, 13, Article 1020827. https://doi.org/10.3389/fendo.2022.1020827
Cleveland Clinic. (n.d.). Endometriosis: Causes, symptoms, diagnosis & treatment. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/10857-endometriosis
Johns Hopkins Medicine. (n.d.). Endometriosis. Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/endometriosis
Macer, M. L., & Taylor, H. S. (2012). Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility. Obstetrics and Gynecology Clinics of North America, 39(4), 535-549. https://doi.org/10.1016/j.ogc.2012.10.002
Maggiore, U. L. R., Chiappa, V., Ceccaroni, M., Roviglione, G., Savelli, L., Ferrero, S., Raspagliesi, F., & Spanò Bascio, L. (2024). Epidemiology of infertility in women with endometriosis. Best Practice & Research Clinical Obstetrics & Gynaecology, 92, Article 102454. https://doi.org/10.1016/j.bpobgyn.2023.102454
Mass General Hospital. (2023). Endometriosis and its impact on fertility. Massachusetts General Hospital. https://www.massgeneral.org/obgyn/fertility/news/endometriosis-and-its-impact-on-fertility
Assessed and Endorsed by the MedReport Medical Review Board